Bipolar Disorder or Drug Use? How Families Can Tell What to Track
Quick answer: It can be very hard to tell from the outside whether a loved one’s behavior is related to bipolar disorder, drug use, alcohol use, or both. Mood symptoms and substance-related changes can overlap. The safest next step is not to diagnose at home. Write down specific observations, avoid accusations, watch for safety risks, and seek help from a qualified professional who can assess both mental health and substance use concerns.
Important note: This article is for general information and caregiver support only. It is not medical, psychiatric, substance use, legal, financial, or emergency advice. It cannot diagnose your loved one. If there is immediate danger, suspected overdose, suicidal language, threats, severe confusion, unsafe driving, violence, or risk to children, contact local emergency services. In the United States, call or text 988 for crisis support.
If someone you love has been acting differently, you may be asking a question that feels almost impossible to answer: is this bipolar disorder, drug use, alcohol use, or both?
The worry is real. The confusion is understandable. Changes in sleep, energy, mood, secrecy, spending, irritability, withdrawal, and risk-taking can show up for many different reasons. From the outside, even a caring spouse, parent, adult child, sibling, or close family member may not be able to tell what is causing the change.
This guide will not tell you whether the behavior is definitely a bipolar mood episode, substance-related, or both. What it can do is help you observe more clearly, avoid harmful assumptions, speak with care, and know when to seek qualified support.
For a broader introduction, you may also find our guide on bipolar disorder and addiction helpful. If this is new territory for your family, you can also start here for bipolar disorder and addiction support.
The Short Answer: It Can Be Hard to Tell From the Outside
Bipolar disorder can involve clear shifts in mood, energy, activity, sleep, concentration, and behavior. Alcohol or other substance use can also affect mood, sleep, judgment, memory, communication, relationships, work, and safety.
Other factors can complicate the picture too. Severe stress, grief, trauma, medical conditions, sleep loss, medication side effects, or another mental health condition can also affect how someone behaves. Family members should not be expected to identify the cause on their own.
This does not mean you should ignore what you are seeing. A safer approach is to slow down, write down facts, keep safety in view, and involve someone qualified to assess the full picture.
Bipolar Disorder, Drug Use, or Both: What Families Should Remember
When you are scared, your mind may search for one explanation. You may want the answer to be clear because uncertainty feels unbearable. With bipolar disorder and substance use concerns, it is often safer to keep more than one possibility open until a professional can assess the situation.
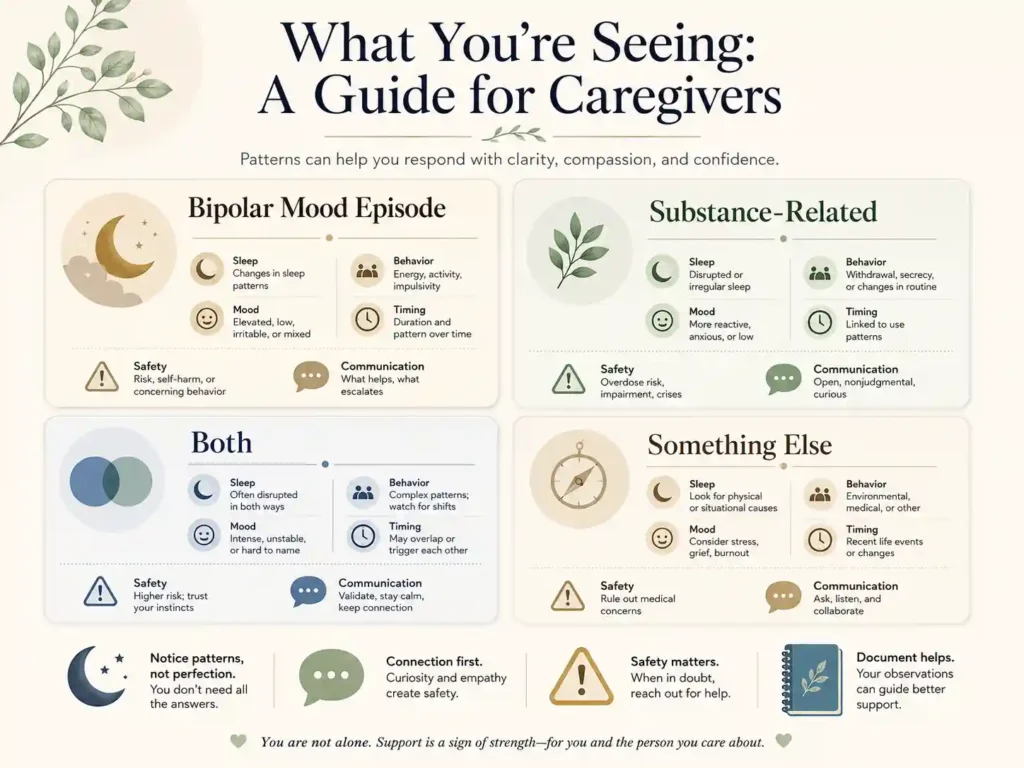
| Possibility | What It Means | What Families Can Do |
|---|---|---|
| It may be a bipolar mood episode | A major change in sleep, energy, mood, judgment, activity, or behavior may be connected to bipolar symptoms. | Track sleep, energy, mood, risk-taking, irritability, spending, speech, and changes from baseline. |
| It may be substance-related | Alcohol or other substances may affect mood, sleep, judgment, memory, secrecy, communication, and safety. | Write down substance-related observations without turning them into accusations. |
| It may be both | Mental health conditions and substance use disorders can occur together, which can make the picture harder to understand. | Ask for support from a provider who can assess both mental health and substance use concerns. |
| It may be something else | Medical issues, trauma, medication effects, stress, grief, or another mental health condition may also affect behavior. | Keep notes factual and seek professional assessment instead of trying to solve the cause alone. |
Why Bipolar Symptoms and Substance Use Can Look Similar
Understanding the overlap can help you respond with more care. It should not be used to diagnose your loved one. The signs below can point in more than one direction, which is exactly why professional assessment matters.
Sleep and Energy Changes
Someone in a manic or hypomanic episode may sleep very little and still seem unusually energized, active, restless, or talkative. Some substances may also affect sleep and energy. Withdrawal from alcohol or other substances can disturb sleep or lead to exhaustion.
A sleep change is important to notice, but it does not prove the cause. The pattern matters more: when it started, how different it is from their usual baseline, and whether it appears together with other changes.
Irritability, Agitation, or Unusual Confidence
Irritability, agitation, increased confidence, defensiveness, or a feeling that others are “against them” can appear during some mood states. Similar changes can also occur with substance use, withdrawal, stress, or sleep deprivation.
Instead of saying, “You are manic” or “You are using,” describe what you have actually noticed.
Try this: “You have seemed more irritable this week, and we have had more conflict than usual. I am worried and want us to get support.”
Risk-Taking, Spending, Driving, Sex, or Conflict
Uncharacteristic risk-taking, impulsive spending, reckless driving, increased sexual behavior, or escalating conflict may happen during a manic or hypomanic episode. These behaviors can also be connected to alcohol or other substance use.
When several changes happen close together, write them down. Dates, examples, amounts, and safety concerns are more useful than conclusions.
Withdrawal, Depression, Shame, or Secrecy
Pulling away from family, sleeping more, losing interest, avoiding conversation, seeming ashamed, or becoming secretive can appear during depression. These changes can also be connected to substance use, withdrawal, fear, shame, or another concern.
Secrecy alone is not proof. A major change in openness, routines, finances, or daily functioning is worth noting carefully.
Confusion, Paranoia, or Behavior That Feels Out of Character
Severe confusion, paranoia, disorientation, or behavior that feels dramatically out of character can be frightening to witness. These changes can happen for different reasons, including mental health episodes, substance effects, withdrawal, medical issues, or severe sleep loss.
When symptoms are severe or safety is at risk, the immediate priority is not figuring out the exact cause. The immediate priority is safety and urgent support.
A Family Observation Checklist
One of the most helpful things you can do is create a factual record. This is not about spying, proving, or building a case against someone. It is about giving a qualified professional a clearer picture.
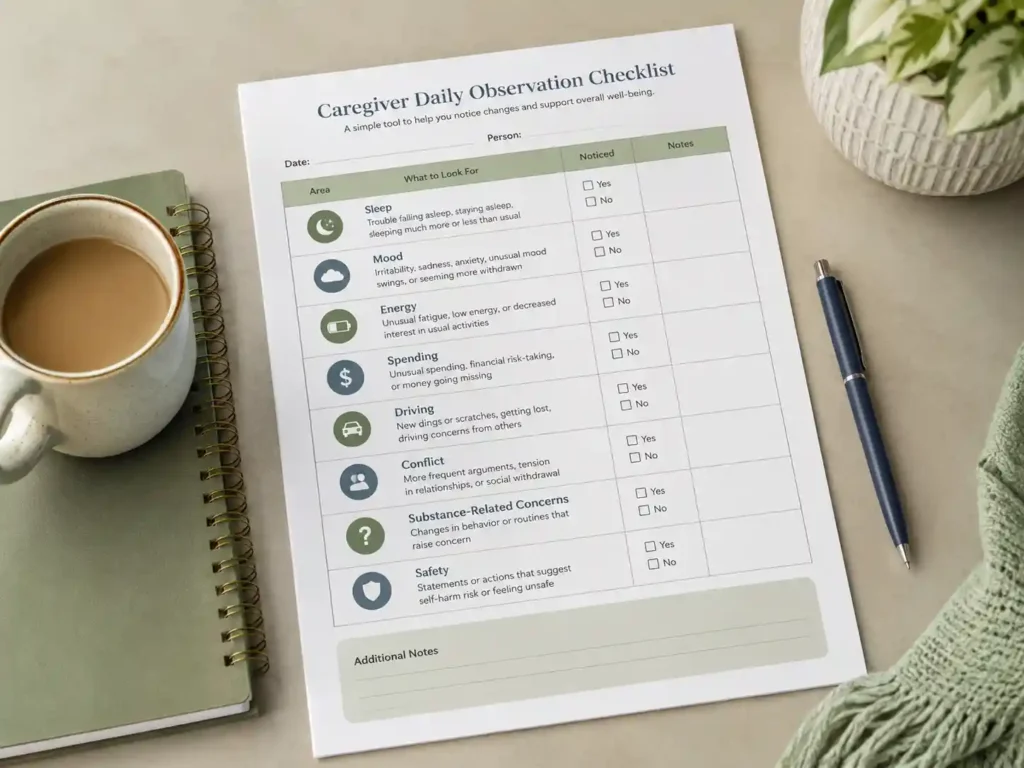
Focus on what you can directly observe:
- Timing: When did the change begin? Was it sudden or gradual? Has it happened before?
- Sleep: Are they sleeping much less or much more than usual?
- Mood and energy: Do they seem unusually energized, irritable, withdrawn, anxious, sad, restless, or agitated?
- Speech and thinking: Are they talking faster, jumping between ideas, making unusually large plans, or saying things that are hard to follow?
- Daily functioning: Has work, parenting, hygiene, eating, school, or household responsibility changed?
- Substance-related concerns: Have you noticed alcohol or other substances, strong smells, missing time, intoxication, withdrawal-like changes, or patterns that concern you?
- Medication context: Has anything changed around prescribed medication, appointments, refills, or side effects? Share this with a professional rather than trying to manage medication yourself.
- Safety concerns: Are there concerns about driving, self-harm, threats, aggression, overdose, children, weapons, or serious financial harm?
Write down dates, facts, and examples. “Slept two hours on Monday and Tuesday, then drove at 2 a.m.” is more useful than “They are out of control.”
Observation Table: Sort What You See Without Diagnosing
The table below is meant to organize what you are noticing. It is not a diagnostic tool. The phrase “could be” is important because each sign can have more than one possible explanation.
| What You Notice | Could Be Mood-Related | Could Be Substance-Related | What to Write Down |
|---|---|---|---|
| Very little sleep, still energized | Could be part of mania or hypomania | Could be related to substance use or withdrawal | Number of nights, hours slept, energy level, and what changed from baseline |
| Sudden or unusual spending | Could be impulsive decision-making during a mood episode | Could be related to purchasing substances or substance-related consequences | Amounts, timing, patterns, and whether household stability is affected |
| Secrecy or missing time | Could be shame, avoidance, or behavior during an episode | Could be hiding use or activities connected to use | When it started, what changed, and whether it is new or recurring |
| Irritability or agitation | Could be part of a manic, mixed, or depressive state | Could be related to intoxication, withdrawal, or substance-related stress | Triggers, intensity, duration, and whether anyone feels unsafe |
| Depression or withdrawal from family | Could be a depressive episode | Could be shame, withdrawal symptoms, or consequences of use | How long it has lasted, what changed, and any words about hopelessness or self-harm |
| Risky driving or near-accidents | Could be poor judgment during a mood episode | Could be impairment or substance-related risk | What you witnessed, when it happened, whether children were present, and whether it repeated |
| Escalating conflict at home | Could be mood instability, irritability, or stress | Could be substance-related agitation or impaired judgment | How often it escalates, what is being said, and whether there are safety concerns |
What to Do First: A Calm Decision Guide
When you are unsure whether this is bipolar disorder, drug use, alcohol use, or both, the first decision is not “Which label is correct?” The first decision is “How safe is this situation right now?”
| Situation | What to Do First | What to Say | What to Avoid |
|---|---|---|---|
| Immediate danger, suicidal language, suspected overdose, violence, threats, or unsafe driving | Seek urgent help. Call emergency services if there is immediate danger. In the United States, call or text 988 for crisis support. | “I care about you. I cannot ignore safety. I am getting help now.” | Do not try to handle a dangerous situation alone. |
| No immediate danger, but behavior has changed quickly | Write down specific observations and choose a calmer time to talk. | “I have noticed changes in sleep, mood, and conflict, and I am worried.” | Do not start with “You are manic” or “You are using.” |
| You suspect substance use but are not sure | Focus on behavior, safety, and support rather than proof. | “I may not understand the cause, but I am worried about what is happening at home.” | Do not search, test, record, or monitor in ways that create safety or legal risks. |
| They already have bipolar disorder and substance use may be involved | Ask for professional help that can assess both concerns. | “Can we talk to someone who understands both mood symptoms and substance use?” | Do not assume only one issue matters. |
| They refuse to discuss support | Set boundaries around unsafe behavior and get support for yourself. | “I cannot force a conversation, but I can decide what I will do to keep the home safe.” | Do not keep absorbing every consequence alone. |
How to Talk Without Accusing
You may not know what is causing the behavior, but you may still need to have a conversation. How you begin matters. A conversation that starts with accusation often becomes a fight about proof. A conversation that starts with concern has a better chance of staying open.
For more help with tone and wording, our guide on communication with someone who has bipolar disorder offers additional support.
Start With Concern, Not Proof
You do not need to prove the cause before you can express concern. You can say what you have noticed, how it is affecting the home, and why you think support would help.
Use “I Noticed” and “I’m Worried” Language
“I noticed you have barely slept this week” is different from “You are manic.” “I am worried about your driving” is different from “You are using again.” The first version gives information. The second version labels or accuses.
Ask About Safety and Support Before Debating the Cause
You and your loved one may not agree on what is happening. Agreement on the label is not always possible at first. You may still be able to agree that the situation is affecting sleep, work, children, money, safety, or the relationship. Start there.
Avoid Labels During the Conversation
Clinical labels, moral labels, and insulting language can close the door quickly. Avoid words that shame, diagnose, or reduce the person to a problem. Describe the behavior and its impact instead.
Calm Scripts You Can Adapt
Scripts can help when emotions are high. Use these as starting points and adjust them to sound like you.
- “I am not trying to accuse you. I am worried because things feel different lately.”
- “I may be wrong about what is causing this, but I want us to get support.”
- “Can we talk to someone who understands both mood symptoms and substance use?”
- “I am willing to listen, but I also need to be honest about what feels unsafe at home right now.”
- “I care about you. I cannot pretend this is not affecting our home.”
- “I do not want to fight about labels. I want us to talk about safety, sleep, and support.”
- “I cannot diagnose what is happening, but I can say that I am worried enough to ask for help.”
For more guidance on supporting without taking over, see how to support someone with bipolar without enabling.
When Both Bipolar Disorder and Substance Use May Need Support
When a mental health condition and a substance use disorder occur together, professionals may describe this as a co-occurring disorder or dual diagnosis. For families, the term matters less than the practical reality: both concerns may need to be assessed.
If only the mood symptoms are discussed, substance-related concerns may be missed. If only the substance use is discussed, mood symptoms may be missed. That is why it can be helpful to ask for support from someone who understands both mental health and substance use concerns.
You do not need to decide which one is “primary” before asking for help. A clear sentence is enough:
“We are seeing mood changes, sleep changes, and possible substance use concerns, and we do not know how to understand them.”
When This Becomes Urgent
Some situations call for immediate support, not careful observation or a planned conversation. Treat the situation as urgent if you notice:
- talk of suicide, self-harm, or wanting to die;
- threats of violence toward others;
- a suspected overdose or signs of severe intoxication;
- severe confusion, disorientation, or loss of contact with reality;
- behavior that puts children in immediate danger;
- reckless driving or another immediate risk of serious injury;
- dangerous access to weapons during escalation;
- severe withdrawal symptoms or a medical emergency.
In these moments, the cause matters less than the immediate safety need. If there is immediate physical danger, contact local emergency services.
A Note About Crisis Support in the United States
In the United States, the 988 Suicide & Crisis Lifeline provides support for people in suicidal crisis or emotional distress. You can call or text 988, or use the chat option at 988lifeline.org. If you are outside the United States, use local emergency or crisis resources for your country.
If this kind of risk has happened before, it may help to create a plan before the next crisis. Our bipolar emergency plan guide can help you think through that process in a calmer moment.
Boundaries That Protect Without Shaming
Boundaries are not punishment. They are a way to protect safety, stability, and emotional health while you seek clarity and support. Whether the concern is bipolar symptoms, substance use, or both, you are allowed to have limits around what happens in your home.
Common areas where boundaries may be needed include conversations during intoxication or severe escalation, driving when safety is questionable, money decisions that affect the household, and children being exposed to unsafe behavior.
Keep boundaries specific and behavior-based. “I will not discuss money while we are both upset” is clearer than “You never act responsibly.” “I cannot allow the kids to ride in the car when I believe driving is unsafe” is clearer than “You are dangerous.”
For more support, see our guides on setting boundaries with someone who has bipolar disorder and what to say when setting boundaries.
If spending, debt, or financial instability is part of the situation, our guide on financial safeguards in a bipolar marriage may be useful. Financial decisions can have legal and practical consequences, so consider qualified financial or legal guidance for your specific situation.
What Not to Do
When you feel scared, it is natural to want certainty and control. Some responses can increase conflict, shame, or risk. The following reminders are offered with compassion, not judgment.
- Do not diagnose your loved one. You can describe what you see, but diagnosis belongs with qualified professionals.
- Avoid starting with accusation. Even if your concern is valid, accusation often leads to defensiveness rather than honesty.
- Do not manage medication. Never tell someone to start, stop, hide, change, ration, or restart medication. Medication decisions should be discussed with qualified providers.
- Avoid unsafe investigation. Do not search, test, record, or monitor in ways that could create safety or legal risks. Seek professional guidance first.
- Skip empty threats. Boundaries should be clear and realistic, not made in panic.
- Do not ignore immediate safety concerns. Relationship conflict and medical uncertainty should not prevent urgent action when someone may be in danger.
- Do not carry this alone. Caregiver isolation can make everything harder. Support for you matters too.
If your loved one refuses to engage with support, our guide on what to do when someone with bipolar refuses help may help you think through your next steps with more calm.
Trusted Resources to Know About
These resources are not a substitute for individualized care, but they can help families find reliable information and support. Always verify current details before relying on any service.
- National Institute of Mental Health: Bipolar Disorder
- National Institute of Mental Health: Substance Use and Mental Health
- SAMHSA: Co-Occurring Disorders
- FindTreatment.gov, a SAMHSA resource for finding mental health and substance use treatment services in the United States and its territories
- SAMHSA National Helpline
- 988 Suicide & Crisis Lifeline
- NAMI: Substance Use Disorders and Co-Occurring Conditions
- NAMI Family Support Group
Next Steps for Caregivers
You do not need to know the full answer before taking a careful next step. Start with what is within your control.
- Write down the facts. Record what happened, when it happened, how long it lasted, and what safety concerns were present.
- Choose a calm moment to talk. Avoid starting a major conversation during intoxication, severe escalation, or a crisis moment.
- Use concern-based language. Focus on what you noticed and why you are worried, not on proving the cause.
- Seek qualified support. This may mean contacting an existing care provider, primary care doctor, mental health clinician, substance use specialist, crisis team, or local support resource.
- Get support for yourself. A therapist, support group, trusted friend, or caregiver resource can help you stay grounded.
- Create a safety plan if risk repeats. If this situation has involved threats, dangerous driving, severe confusion, overdose concerns, or risk to children, do not wait until the next crisis to think through your options.
Helpful Tools for This Guide
- Observation sentence: “I am going to write down facts, not conclusions.”
- Conversation sentence: “I may not know the cause, but I am worried about the pattern.”
- Safety sentence: “This is bigger than a family argument. I am getting outside help.”
- Boundary sentence: “I cannot control the diagnosis, but I can set limits around unsafe behavior.”
- Support sentence: “I need someone qualified to help us look at both mood symptoms and substance use concerns.”
For More Calm Caregiver Support
If you are trying to support someone with bipolar disorder while also protecting your own stability, consider joining our caregiver newsletter. You will receive practical scripts, boundary reminders, observation tools, and crisis-planning resources written for families who need calm support without fear-based language.
Frequently Asked Questions
Can drug use look like bipolar disorder?
Yes. Changes in sleep, energy, mood, behavior, and risk-taking can appear in connection with alcohol or other substance use, and similar changes can appear during mood episodes related to bipolar disorder. From the outside, the two can be difficult to distinguish without a comprehensive assessment. Professional evaluation is important rather than family interpretation.
Can alcohol use look like bipolar symptoms?
Alcohol use, intoxication, withdrawal, or alcohol-related stress can affect sleep, mood, judgment, memory, irritability, secrecy, and family conflict. Some of these changes can overlap with bipolar symptoms. A family member may notice patterns, but a qualified professional should assess the cause.
Can someone have both bipolar disorder and a substance use problem?
Yes. Mental health conditions and substance use disorders can occur together. When they do, each concern can affect how the other appears, which can make assessment more complex. A qualified provider can help determine what kind of support is appropriate.
How can I tell if it is mania or drug use?
You may not be able to tell from the outside. Mania, substance use, withdrawal, sleep loss, stress, or another health issue can all affect behavior. Write down observable facts such as sleep changes, spending, speech, driving, conflict, substance-related concerns, and safety risks. Then share those facts with a qualified professional.
Should I confront my loved one if I suspect drug use?
Leading with accusation or proof often creates defensiveness. A calmer approach starts with concern and uses language such as “I noticed” and “I am worried.” You can be honest about what you have seen and how it affects the home without arriving with a verdict.
What should I write down before asking for professional help?
Focus on facts rather than interpretations. Write down what you observed, when it started, how it differs from their usual baseline, any patterns in timing or behavior, and specific safety concerns. Include notes about sleep, mood, energy, spending, secrecy, driving, conflict, and any substance-related observations.
What should I avoid doing if I suspect both bipolar symptoms and substance use?
Avoid diagnosing, shaming, threatening, secretly managing medication, or investigating in ways that could create legal or safety risks. Focus on safety, clear observations, calm communication, and professional support. If there is immediate danger, seek urgent help.
When should I treat this as urgent?
Treat the situation as urgent if there is talk of suicide or self-harm, threats toward others, suspected overdose, severe confusion or disorientation, behavior that puts children in immediate danger, or dangerous driving. If there is immediate physical danger, contact local emergency services. In the United States, the 988 Suicide & Crisis Lifeline can also provide crisis support.
Related Guides for Families
- Bipolar Disorder and Addiction: A Family Guide
- Start Here: Bipolar Disorder and Addiction Support
- What to Do When Someone With Bipolar Refuses Help
- How to Create a Bipolar Emergency Plan
- How to Support Someone With Bipolar Without Enabling
- How to Communicate With Someone Who Has Bipolar Disorder
- Setting Boundaries With Someone Who Has Bipolar Disorder
- Bipolar Caregiver Burnout: Signs, Checklist, and Recovery Plan
Final Takeaway
Trying to tell the difference between bipolar disorder, drug use, alcohol use, or both can leave families feeling trapped between fear and uncertainty. You may want a clear answer before you act, but the safer first step is often simpler: observe carefully, speak without accusation, protect safety, and bring in qualified support.
You do not have to diagnose your loved one to say, “Something has changed, and I am worried.” You do not have to prove the cause before asking for help. A factual record, calm language, and a safety-aware plan can help you move from panic toward a clearer next step.
Read next: Bipolar Disorder and Addiction: A Family Guide, What to Do When Someone With Bipolar Refuses Help, and How to Create a Bipolar Emergency Plan.