Types of Bipolar Disorder: What Families Should Know
Author: Elena, Caregiver Advocate. Last reviewed: July 6, 2026
Educational information only. This article does not replace professional evaluation, diagnosis, treatment, or crisis care.
Quick answer: The main types of bipolar disorder include Bipolar I disorder, Bipolar II disorder, cyclothymic disorder, and other specified or unspecified bipolar and related disorders. The difference is not simply “more severe” or “less severe.” Clinicians look at the pattern of mania, hypomania, depression, duration, impairment, safety risk, and whether psychosis or hospitalization has occurred. Families should not diagnose the type at home. They can help by tracking sleep, mood, energy, behavior, safety concerns, and the impact on daily life.
Important safety note: If someone is talking about suicide, self-harm, harming others, behaving violently, experiencing psychosis, driving unsafely, using substances in a dangerous way, or seems unable to stay safe, seek urgent help. In the United States, call or text 988 for mental health crisis support. If there is immediate danger, contact local emergency services.
When families search for the types of bipolar disorder, they are usually trying to understand what a diagnosis means, why symptoms look different from person to person, and what they should watch for at home. One person may have dramatic manic episodes. Another may mostly struggle with depression and only brief periods of hypomania. Someone else may have chronic mood ups and downs that never fit neatly into a single episode.
This guide explains the main bipolar disorder types in plain English, with a caregiver focus. You will learn how Bipolar I, Bipolar II, cyclothymia, mixed features, and rapid cycling differ, what families can safely track, and when symptoms should become urgent.
If you are still trying to understand warning signs, start with early signs of bipolar disorder. If symptoms are already affecting safety, money, work, parenting, or relationships, read untreated bipolar disorder: risks and safe next steps.
Quick Answer: What Are the Main Types of Bipolar Disorder?
Bipolar disorder is a mood disorder that can involve episodes of mania, hypomania, depression, mixed symptoms, sleep disruption, changes in energy, and changes in judgment or functioning. The “type” depends on the pattern of mood episodes over time.
| Type | Core Pattern | What Families May Notice | Why It Matters |
|---|---|---|---|
| Bipolar I disorder | At least one manic episode. Depressive episodes often happen but are not required for diagnosis. | Very little sleep, high energy, impulsive decisions, risky behavior, agitation, grand plans, psychosis, or hospitalization risk. | Mania can become dangerous or severely impairing and may require urgent care. |
| Bipolar II disorder | At least one hypomanic episode and at least one major depressive episode, with no full manic episode. | Long depression, periods of higher energy, less sleep, irritability, productivity, impulsivity, or behavior that feels out of character. | Depression can be severe, and hypomania can be missed because it may look like functioning well. |
| Cyclothymic disorder | Long-term mood ups and downs with hypomanic symptoms and depressive symptoms that do not meet full episode criteria. | Ongoing mood fluctuation, emotional reactivity, energy changes, relationship strain, and inconsistent functioning. | The pattern may feel “normal” to the person but still disrupt life over time. |
| Other specified or unspecified bipolar and related disorders | Bipolar-like symptoms that cause distress or impairment but do not fit neatly into Bipolar I, Bipolar II, or cyclothymia. | Shorter mood episodes, incomplete patterns, confusing symptoms, or symptoms affected by substances, medical issues, or other conditions. | Careful follow-up matters because patterns can become clearer over time. |
This table is a plain-English guide, not a diagnostic tool. A qualified clinician needs to evaluate the full history, symptoms, safety risk, medical factors, substance use, and functioning.
Why Bipolar Type Matters for Families
The type of bipolar disorder can affect the treatment plan, safety planning, medication discussions, follow-up needs, and what families should watch for. It can also help caregivers understand why one person’s bipolar disorder does not look like another person’s.
For example, a family caring for someone with Bipolar I may be more focused on manic warning signs, psychosis, unsafe behavior, spending, and crisis planning. A family caring for someone with Bipolar II may be more focused on depression, missed responsibilities, suicidal thoughts, and subtle hypomania that others may praise as “productive.”
The label matters, but the daily pattern matters too. Families should pay attention to:
- how sleep changes before symptoms worsen;
- whether energy rises or crashes;
- whether mood shifts are euphoric, irritable, depressed, mixed, or anxious;
- whether judgment changes around money, driving, sex, substances, conflict, or work;
- whether psychosis, paranoia, hallucinations, or severe confusion appear;
- whether the person can still function safely at home, work, school, or as a parent;
- whether symptoms repeat, escalate, or become more dangerous.
If the person has not been evaluated yet, your role is not to choose the diagnosis. Your role is to describe what you are seeing clearly enough for a professional to assess it.
Bipolar I Disorder
Bipolar I disorder is defined by at least one manic episode. Depressive episodes are common in Bipolar I, but a major depressive episode is not required for the diagnosis.
What mania can look like
A manic episode is more than being energetic, happy, or productive. It usually involves a noticeable change in mood and energy that affects functioning, judgment, sleep, and behavior. Mania may include elevated mood, extreme irritability, grandiosity, racing thoughts, fast speech, less need for sleep, impulsive choices, agitation, psychosis, or unsafe behavior.
| Mania Sign | What Families May Notice | Why It Can Become Urgent |
|---|---|---|
| Reduced need for sleep | The person sleeps very little for several nights but does not seem tired. | No sleep with rising energy can quickly affect judgment, safety, and conflict. |
| Grand plans or grandiosity | They feel unusually powerful, chosen, invincible, or certain they can do impossible things. | Grandiosity may lead to risky money, work, travel, legal, or relationship decisions. |
| Impulsive behavior | Spending, risky driving, substance use, unsafe sex, quitting jobs, or sudden travel. | Consequences can affect safety, debt, legal risk, health, and family stability. |
| Fast speech or racing thoughts | They talk rapidly, jump topics, interrupt often, or cannot slow down. | It may become hard to communicate, de-escalate, or make safe decisions together. |
| Psychosis or severe confusion | Paranoia, hallucinations, delusions, or losing touch with reality. | This should be treated as urgent and may require crisis support or emergency care. |
What families should remember about Bipolar I
Bipolar I is not defined by personality, character, or “being dramatic.” It is defined by a history of mania. During mania, a person may not fully understand how unsafe or unusual their behavior looks from the outside. Families often need a plan before symptoms escalate.
Helpful next guides: how to create a bipolar emergency plan and what to say during a manic episode.
Bipolar II Disorder
Bipolar II disorder involves at least one hypomanic episode and at least one major depressive episode. A person with Bipolar II has not had a full manic episode. This distinction matters because hypomania can be subtle, while depression can be very impairing.
Why Bipolar II is often missed
Hypomania may look like confidence, productivity, charm, social energy, creativity, or finally “feeling better” after depression. Because it may not cause obvious crisis at first, the person may not report it to a clinician. Families may remember it only later, after repeated cycles become clearer.
Bipolar II should not be dismissed as “mild bipolar.” Depression in Bipolar II can be severe and may affect work, school, parenting, relationships, hygiene, appetite, sleep, and safety.
| Bipolar II Pattern | What It Can Look Like | What Families Can Track |
|---|---|---|
| Hypomania | Less sleep, higher energy, more talking, more ideas, irritability, impulsivity, or intense productivity. | Sleep hours, energy level, spending, risk-taking, work changes, relationship conflict, and later crashes. |
| Major depression | Low mood, hopelessness, withdrawal, fatigue, poor concentration, missed responsibilities, or loss of interest. | Duration, severity, hygiene, appetite, missed work or school, suicidal language, and functioning. |
| Post-hypomania crash | A period of energy and confidence is followed by exhaustion, shame, sadness, or depression. | What happened before the crash, how long it lasted, and whether safety was affected. |
| Subtle impairment | The person seems functional to others but unstable at home or in close relationships. | Private consequences: bills, parenting strain, conflict, missed sleep, secrecy, and emotional volatility. |
If depression is the most visible symptom, families may also find it helpful to read bipolar disorder medication types: what families should know, especially the sections about bipolar depression and prescriber questions.
Cyclothymic Disorder
Cyclothymic disorder, also called cyclothymia, involves long-term mood fluctuation with periods of hypomanic symptoms and depressive symptoms that do not meet full criteria for hypomanic or major depressive episodes. Even when symptoms are less extreme than Bipolar I or Bipolar II, the pattern can still affect relationships, work, school, trust, and daily stability.
What cyclothymia can feel like at home
Families may describe the person as unpredictable, sensitive, reactive, energetic for a while, then low, withdrawn, or discouraged. The person may feel that this is “just how I am,” especially if the pattern has existed for years.
| Possible Cyclothymic Pattern | How It May Affect the Family | Helpful Response |
|---|---|---|
| Frequent mood shifts | The home feels emotionally unpredictable even without a clear crisis. | Track patterns over time instead of reacting to each mood change as a separate event. |
| Periods of higher energy | More plans, more intensity, more irritability, or less sleep. | Watch sleep, conflict, spending, and whether energy is rising beyond the person’s usual baseline. |
| Periods of depressive symptoms | Withdrawal, low motivation, sadness, fatigue, or feeling defeated. | Take depressive symptoms seriously, especially if hopelessness or self-harm language appears. |
| Long-term relationship strain | Partners or relatives may feel confused by repeated ups and downs. | Use clear boundaries, predictable routines, and professional support rather than blame. |
Cyclothymia can be easy to minimize because it may not look like the dramatic version of bipolar disorder many people imagine. But chronic instability still deserves evaluation and support.
Other Specified or Unspecified Bipolar and Related Disorders
Sometimes a person has bipolar-like symptoms that cause real distress or impairment but do not fit neatly into Bipolar I, Bipolar II, or cyclothymic disorder. Clinicians may use categories such as other specified bipolar and related disorder or unspecified bipolar and related disorder.
This does not mean the symptoms are fake or unimportant. It usually means the pattern needs careful clinical judgment, more history, or more time to understand clearly.
Why this category can be confusing for families
- Symptoms may be shorter than typical episode descriptions.
- Depression may be clear, but hypomanic symptoms may be subtle.
- Substance use, trauma, sleep deprivation, medication effects, or medical issues may complicate the picture.
- The person may have strong symptoms but not enough information yet for a more specific diagnosis.
- The diagnosis may change after better history, follow-up, or mood tracking.
If alcohol or drug use may be involved, read bipolar disorder or drug use: what families can track. If your loved one is refusing evaluation, read what to do when someone with bipolar refuses help.
Bipolar Types Compared
The easiest way to understand the differences is to compare the mood episode pattern. This table is designed for families, not clinicians. It helps you understand the language you may hear during evaluation.
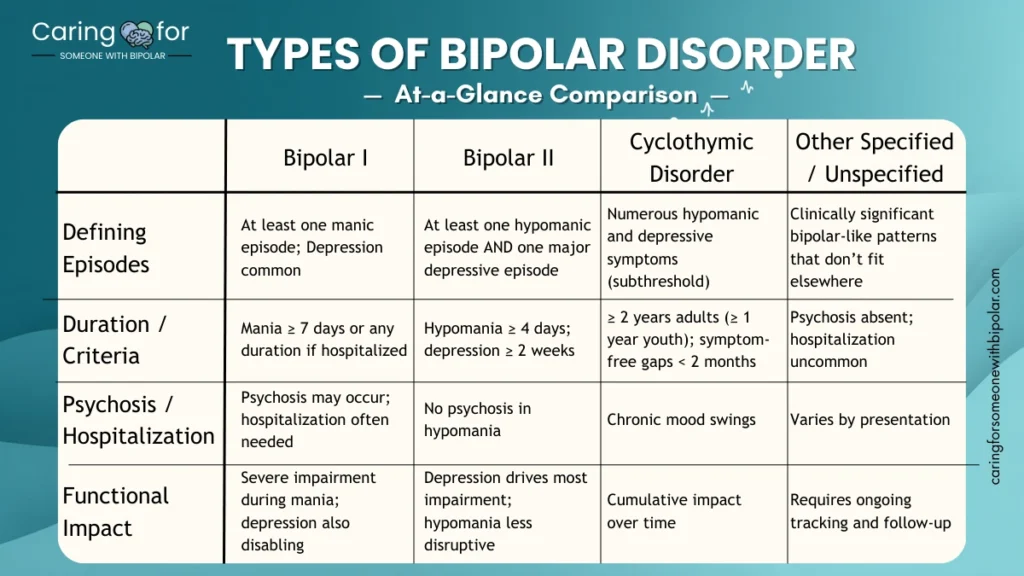
| Feature | Bipolar I | Bipolar II | Cyclothymic Disorder | Other Specified / Unspecified |
|---|---|---|---|---|
| Mania | At least one manic episode is required. | No history of full mania. | No full manic episode. | May have bipolar-like symptoms that do not meet full criteria. |
| Hypomania | May happen, but mania defines the diagnosis. | At least one hypomanic episode is required. | Hypomanic symptoms occur repeatedly but do not meet full episode criteria. | May be shorter, unclear, or part of a mixed pattern. |
| Depression | Common, but not required for diagnosis. | At least one major depressive episode is required. | Depressive symptoms occur repeatedly but do not meet full major depression criteria. | May be present, unclear, or part of a partial pattern. |
| Psychosis | Can occur during mania or severe depression. | Psychosis is not part of hypomania. If psychosis appears during elevated mood, clinicians reassess the diagnosis. | Not typical. | Varies and needs professional evaluation. |
| Safety concerns | May be high during mania, psychosis, severe agitation, or impulsive behavior. | Often high during depression, suicidal thoughts, or impulsive hypomanic behavior. | Usually chronic strain, but safety risk still matters if depression or impulsivity worsens. | Depends on symptoms, substances, sleep loss, psychosis, and impairment. |
| What families should track | Sleep, mania signs, psychosis, spending, risk-taking, aggression, and crisis patterns. | Depression, hypomania, sleep, irritability, impulsivity, and post-high crashes. | Long-term mood fluctuation, sleep, energy, conflict, and functioning. | Dates, duration, triggers, symptoms, substances, medical factors, and safety concerns. |
Mania, Hypomania, Depression, and Mixed Features
The bipolar type depends heavily on the difference between mania, hypomania, depression, and mixed features. Families do not need to diagnose these states, but understanding the words can make appointments less confusing.
| Term | Plain-English Meaning | What Families May Notice | Why It Matters |
|---|---|---|---|
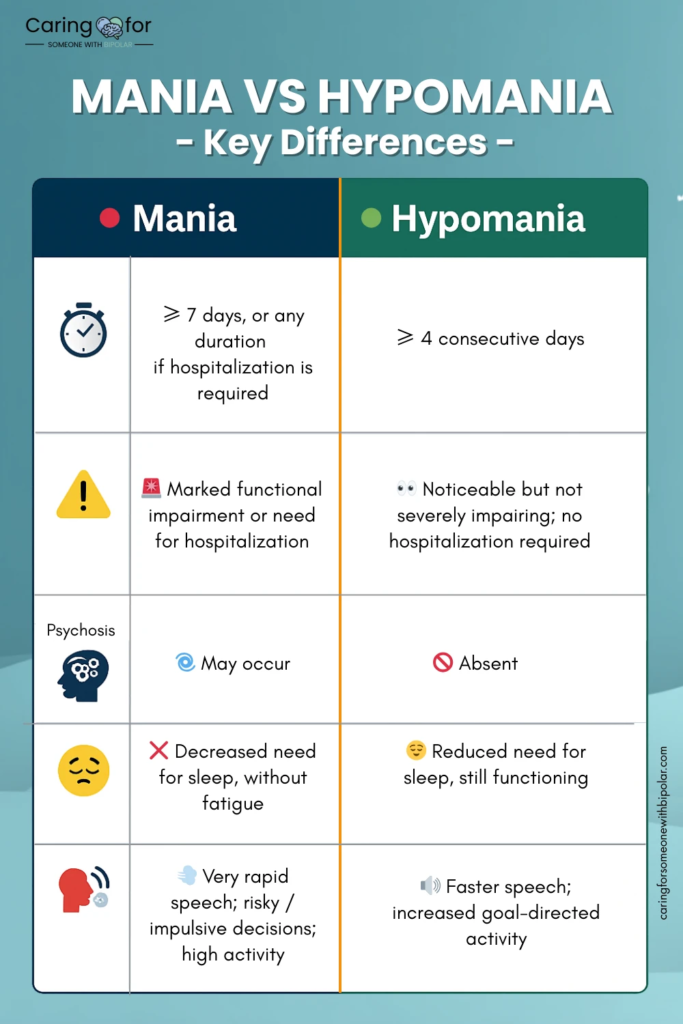
| Mania | A high-energy mood episode that causes major impairment, safety risk, psychosis, or hospitalization risk. | No sleep, racing thoughts, grand plans, risky behavior, agitation, psychosis, or severe conflict. | Mania can become urgent and often requires professional care quickly. |
| Hypomania | A less severe high-energy episode that is noticeable but not as impairing as mania. | More energy, less sleep, confidence, irritability, productivity, talkativeness, or impulsivity. | It may be missed because it can look positive at first. |
| Depression | A low mood episode that affects motivation, sleep, concentration, hope, and daily functioning. | Withdrawal, fatigue, sadness, hopelessness, missed responsibilities, poor hygiene, or suicidal language. | Depression can be dangerous, especially when hopelessness or self-harm thoughts appear. |
| Mixed features | Symptoms of depression and mania or hypomania appear together. | Depressed but agitated, hopeless but unable to sleep, energized but distressed, irritable, impulsive, or restless. | Mixed symptoms can feel confusing and may increase safety concerns. |
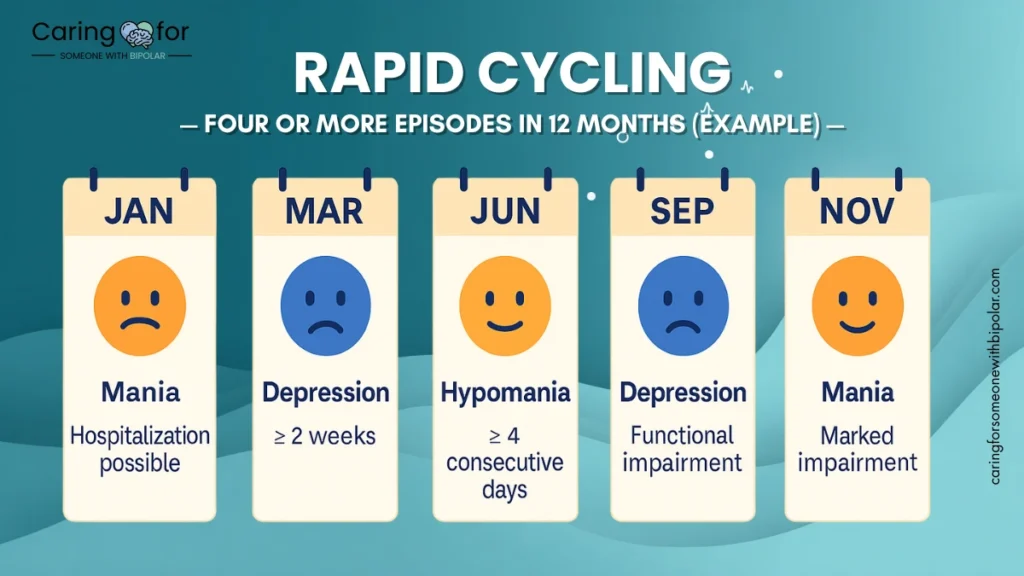
| Rapid cycling | Multiple mood episodes occur within a year. | Repeated highs, lows, mixed symptoms, crashes, or unstable periods. | Tracking dates and patterns becomes especially important. |
Mixed symptoms can be especially confusing for families because the person may look depressed and energized at the same time. For example, they may feel hopeless but also restless, sleepless, impulsive, or agitated. This is one reason safety planning matters even when the person does not look “manic” in the obvious sense.
What Families Can Safely Track
Families can support an evaluation by bringing factual observations, not arguments or labels. Instead of saying “They are Bipolar I” or “They are hypomanic,” write down what happened, when it happened, how long it lasted, and whether it affected safety or functioning.
| What to Track | Examples to Write Down | Why It Helps the Clinician |
|---|---|---|
| Sleep | Bedtime, wake time, nights with little sleep, sleeping too much, all-nighters. | Sleep changes are often central to mood episodes. |
| Energy and activity | Unusual productivity, pacing, starting many projects, sudden exhaustion, crashes. | Energy change helps separate mood episodes from ordinary stress. |
| Mood | Elevated mood, irritability, anger, sadness, hopelessness, emotional sensitivity. | Mood pattern helps clarify mania, hypomania, depression, or mixed symptoms. |
| Speech and thoughts | Fast speech, jumping topics, racing thoughts, confusion, unusual beliefs. | These details can show how severe or impairing the episode may be. |
| Judgment and behavior | Spending, driving, substances, sex, conflict, sudden travel, quitting work, legal risks. | Behavioral changes help show impairment and safety risk. |
| Depression and safety | Withdrawal, missed responsibilities, self-harm language, talk of death, feeling like a burden. | Safety concerns should be taken seriously and may need urgent support. |
| Substances and medical factors | Alcohol, drugs, medication changes, illness, postpartum changes, sleep deprivation. | These can affect mood and must be discussed with a professional. |
Use neutral language. “Slept two hours for three nights and spent $900 online” is more useful than “acted crazy.” “Stayed in bed for five days and said life is pointless” is more useful than “lazy.” Facts help. Labels usually create defensiveness.
What Bipolar Type Does Not Tell You
The diagnosis type can be helpful, but it does not tell the whole story. Two people with the same bipolar type can have very different symptoms, risks, treatment plans, family needs, and recovery paths.
The type does not automatically tell you:
- how kind, responsible, or trustworthy the person is;
- whether the person will accept treatment;
- whether they will need medication, therapy, hospitalization, or a different level of support;
- whether they can parent, work, study, or maintain relationships;
- whether symptoms are caused only by bipolar disorder;
- how severe the next episode will be;
- what boundaries your family needs.
This is why families should combine diagnosis education with practical planning. For boundaries and support, see how to support someone with bipolar without enabling and setting boundaries with someone who has bipolar disorder.

Diagnosis: What to Expect
There is no simple home test that can confirm the type of bipolar disorder. A professional evaluation may include a detailed history of mood episodes, sleep, energy, depression, family history, substance use, medical conditions, medication reactions, trauma, functioning, and safety.
The clinician may ask about:
- past periods of mania or hypomania;
- past depressive episodes;
- how long symptoms lasted;
- whether symptoms caused impairment, psychosis, or hospitalization;
- sleep changes during high-energy periods;
- substance use or withdrawal;
- medical conditions or medications that could affect mood;
- family history of mood disorders;
- suicidal thoughts, self-harm, aggression, or unsafe behavior.
If symptoms are still early or unclear, the clinician may continue to assess the pattern over time. A mood diary, family observations, and past records can help.
Children, Teens, and Bipolar Types
Bipolar disorder in children and teens can be harder to evaluate because symptoms may overlap with ADHD, depression, anxiety, trauma, autism, substance use, disruptive behavior, or normal developmental changes. Families should be careful about labeling a young person too quickly.
Seek a professional evaluation if you notice intense mood changes, severe sleep disruption, risky behavior, depression, rage, psychosis, self-harm language, or functioning problems at school, home, or with peers.
If children in the home are affected by a parent’s symptoms, read supporting children of bipolar parents.
When to Seek Urgent Help
Some situations should not wait for a routine appointment. Seek urgent professional support if symptoms involve safety, psychosis, severe confusion, or risk of harm.
| Urgent Concern | Examples | What to Do |
|---|---|---|
| Suicide or self-harm risk | Talking about death, wanting to disappear, feeling like a burden, self-harm, or preparing for suicide. | Use crisis support immediately. In the U.S., call or text 988. If danger is immediate, call emergency services. |
| Psychosis or severe confusion | Hallucinations, delusions, paranoia, not making sense, or losing touch with reality. | Seek urgent clinical or emergency support. |
| No sleep with escalating behavior | Several nights with little or no sleep plus impulsivity, agitation, grandiosity, or unsafe decisions. | Do not wait for the situation to “burn out.” Contact a clinician or crisis support. |
| Threats or violence | Threats toward self or others, physical aggression, weapons, unsafe driving, or severe agitation. | Prioritize safety. Leave the situation if needed and contact emergency support. |
| Dangerous substance use | Overdose risk, mixing substances, intoxication with mood symptoms, or withdrawal concerns. | Seek urgent medical or crisis support and mention both mood symptoms and substance concerns. |
A crisis plan is easier to use when it is written before the emergency. See how to create a bipolar emergency plan.
How to Talk About Bipolar Types Without Starting a Fight
Families often want to say, “You have Bipolar I” or “This is Bipolar II.” That may be understandable, but it often leads to defensiveness. A calmer approach is to describe patterns and suggest professional support.
| Avoid Saying | Try Saying Instead | Why It Helps |
|---|---|---|
| “You are definitely bipolar.” | “I noticed big changes in sleep, energy, and mood. I think it would help to talk with someone qualified.” | It avoids diagnosing and focuses on observable facts. |
| “You are manic.” | “You slept very little this week and seem more energized and impulsive than usual. I am worried.” | It reduces shame and gives specific information. |
| “You are just depressed again.” | “You seem really low and withdrawn, and I want us to take that seriously.” | It validates depression without minimizing it. |
| “You need medication.” | “Can we write down what has changed and ask a prescriber what options are safe?” | It keeps medical decisions with professionals. |
| “You are ruining everything.” | “I care about you, and I also need us to protect sleep, safety, money, and the kids.” | It combines compassion with boundaries. |
For more wording help, read how to communicate with someone who has bipolar disorder and what not to say to someone with bipolar disorder.
Related Guides for Families
- Early Signs of Bipolar Disorder: What Families Should Track
- Untreated Bipolar Disorder: Risks and Safe Next Steps
- Bipolar Disorder Medication Types: What Families Should Know
- How to Create a Bipolar Emergency Plan
- What to Do When Someone With Bipolar Refuses Help
- Bipolar Disorder or Drug Use? What Families Can Track
- How to Support Someone With Bipolar Without Enabling
- Supporting Children of Bipolar Parents
Trusted Resources
These resources can help families learn more and prepare for professional support. They do not replace individualized medical care.
- National Institute of Mental Health: Bipolar Disorder
- NIMH: Bipolar Disorder Topic Page
- NIMH: Bipolar Disorder in Children and Teens
- NAMI: Bipolar Disorder
- Mayo Clinic: Bipolar Disorder Symptoms and Causes
- Mayo Clinic: Cyclothymia
- SAMHSA: 988 Suicide & Crisis Lifeline
- 988 Suicide & Crisis Lifeline
Frequently Asked Questions About Types of Bipolar Disorder
What are the main types of bipolar disorder?
The main types include Bipolar I disorder, Bipolar II disorder, cyclothymic disorder, and other specified or unspecified bipolar and related disorders. The type depends on the pattern of mania, hypomania, depression, duration, impairment, and safety concerns.
What is the difference between Bipolar I and Bipolar II?
Bipolar I involves at least one manic episode. In Bipolar II, the pattern includes at least one hypomanic episode and at least one major depressive episode, with no full manic episode. This does not mean Bipolar II is simply a mild version of Bipolar I, because depression can still be severe and disabling.
Is Bipolar I more serious than Bipolar II?
Bipolar I can involve severe mania, psychosis, hospitalization, or dangerous behavior. Bipolar II can involve severe depression, suicide risk, and major impairment. Both can be serious and both deserve professional care.
What is cyclothymic disorder?
Cyclothymic disorder, or cyclothymia, is a long-term pattern of mood ups and downs involving hypomanic symptoms and depressive symptoms that do not meet full criteria for hypomanic or major depressive episodes. It can still disrupt relationships, work, school, and daily life.
Can bipolar disorder include mixed features?
Yes. Mixed features mean symptoms of depression and mania or hypomania can appear together. A person may feel depressed but also restless, sleepless, agitated, impulsive, or full of racing thoughts. Mixed symptoms can be confusing and may raise safety concerns.
What is rapid cycling in bipolar disorder?
Rapid cycling generally means a person has multiple mood episodes within a year. Families can help by tracking dates, sleep changes, depression, mania or hypomania signs, and what happened before each episode.
Can the bipolar type change over time?
A diagnosis may be clarified over time as more information becomes available. For example, if someone previously diagnosed with Bipolar II later has a full manic episode, a clinician may reassess the diagnosis. Families should share clear observations with the treatment team.
Can someone have bipolar symptoms that do not fit a clear type?
Yes. Some people have bipolar-like symptoms that cause distress or impairment but do not fit neatly into Bipolar I, Bipolar II, or cyclothymia. A clinician may use other specified or unspecified bipolar and related disorder while continuing to assess the pattern.
How can families help without diagnosing?
Families can track sleep, mood, energy, behavior, spending, substances, depressive symptoms, psychosis, and safety concerns. Use dates and examples instead of labels. Encourage professional evaluation and support.
When should bipolar symptoms become urgent?
Seek urgent help if there is suicidal language, self-harm, threats, violence, psychosis, severe confusion, unsafe driving, dangerous substance use, or no sleep for days with escalating impulsivity or agitation.
Final Takeaway
Understanding the types of bipolar disorder can help families respond with more clarity and less panic. Bipolar I, Bipolar II, cyclothymia, and other bipolar-related diagnoses are based on patterns of mood episodes, not personality or character.
You do not need to diagnose your loved one at home. The most helpful thing you can do is track what changes, protect safety, encourage professional evaluation, and build a support plan that does not depend on one exhausted caregiver doing everything alone.
Start with the basics: sleep, mood, energy, behavior, safety, and functioning. Those patterns are often more useful than arguments about labels.