Early Signs of Bipolar Disorder: What Families Should Track
Quick answer: Early signs of bipolar disorder can include noticeable changes in sleep, energy, mood, speech, activity, judgment, irritability, spending, risk-taking, concentration, and periods of depression. Families should not try to diagnose bipolar disorder at home. The safest first step is to track clear patterns over time, watch for safety concerns, and encourage a professional evaluation.
Important safety note: If someone is talking about suicide, self-harm, harming others, behaving violently, experiencing psychosis, driving unsafely, using substances in a dangerous way, or seems unable to stay safe, seek urgent help. In the United States, call or text 988 for crisis support. If there is immediate danger, contact local emergency services.
The early signs of bipolar disorder are often confusing because they can look like stress, burnout, anxiety, depression, ADHD, personality changes, substance use, or normal life pressure. A person may sleep less and seem energized for a while, then crash into exhaustion or depression. They may become unusually talkative, irritable, impulsive, withdrawn, or emotionally intense.
This guide is written for families, partners, parents, and caregivers who are trying to understand what they are seeing without labeling the person or escalating conflict. You will learn what signs to track, what may suggest mania or hypomania, what bipolar depression can look like, what can overlap with bipolar disorder, and when support becomes urgent.
If you are still learning the basics, read types of bipolar disorder. If symptoms are already affecting safety, money, relationships, parenting, work, or school, read untreated bipolar disorder: risks and safe next steps.
What Are Early Signs of Bipolar Disorder?
Early signs are not always dramatic. They are often patterns that become clearer when you look at sleep, mood, energy, behavior, and daily functioning over days or weeks.
| Area to Watch | What Families May Notice | What to Track | When to Seek Help Faster |
|---|---|---|---|
| Sleep | Sleeping very little without seeming tired, or sleeping much more than usual. | Bedtime, wake time, total sleep, naps, all-nighters, early waking. | No sleep or very little sleep with rising energy, agitation, impulsivity, or unsafe behavior. |
| Energy | Sudden bursts of energy, pacing, restlessness, intense productivity, or sudden exhaustion. | Energy level, activity level, new projects, physical restlessness, crashes. | Energy becomes intense, risky, aggressive, or paired with poor judgment. |
| Mood | Unusual confidence, euphoria, irritability, sadness, anger, or emotional sensitivity. | Mood changes, triggers, duration, intensity, and whether the mood fits the situation. | Extreme mood changes, threats, suicidal language, or behavior that feels unsafe. |
| Speech and thoughts | Talking faster, jumping topics, racing thoughts, or difficulty slowing down. | Speech speed, topic changes, pressured talking, confusion, unusual beliefs. | Severe confusion, paranoia, hallucinations, or inability to communicate clearly. |
| Judgment | Spending, risky driving, impulsive travel, quitting plans, unsafe sex, or conflict. | Money decisions, driving, substances, relationship conflict, legal or work risks. | Any behavior that could lead to harm, debt, violence, arrest, or exploitation. |
| Depression | Withdrawal, hopelessness, fatigue, poor hygiene, missed work, or loss of interest. | Isolation, appetite, sleep, hygiene, missed responsibilities, self-critical words. | Talk of death, self-harm, feeling like a burden, or having no reason to live. |
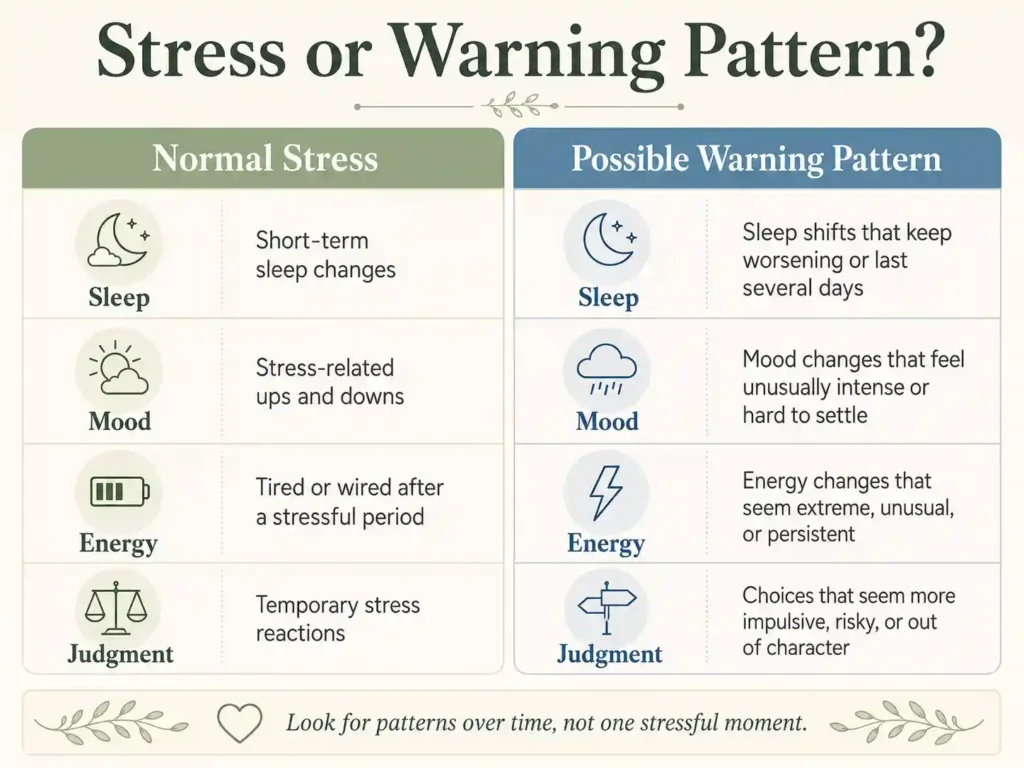
Early Signs vs Normal Mood Changes
Everyone has hard days, emotional reactions, bursts of motivation, or periods of sadness. The concern is not one mood change by itself. The concern is a pattern that is intense, repeated, difficult to explain, or damaging to safety and daily life.
| Normal Stress or Mood Shift | Possible Warning Pattern | Helpful Family Response |
|---|---|---|
| Staying up late for a deadline and feeling tired the next day. | Sleeping only a few hours for several nights while feeling energized or unstoppable. | Track sleep and gently encourage rest and professional support if it continues. |
| Feeling excited about a new idea. | Starting many urgent projects, spending impulsively, or making big plans that feel out of character. | Write down specific behavior without arguing about labels. |
| Being irritable during a stressful week. | Irritability that escalates into rage, threats, unsafe driving, or major conflict. | Prioritize safety and avoid trying to win the argument. |
| Feeling sad after disappointment. | Long withdrawal, hopelessness, missed responsibilities, or talk of death. | Take depression seriously and seek support sooner. |
| Having a productive season. | Productivity paired with reduced sleep, racing thoughts, impulsivity, or grand plans. | Track the pattern and suggest a professional evaluation. |
How Bipolar Disorder Can Begin
Bipolar disorder does not always appear as a sudden crisis. For some people, early patterns build gradually. Families may first notice sleep disruption, emotional intensity, depression, irritability, changes in confidence, impulsive choices, or shifts in functioning.
Some people first seek help during depression. Others may not recognize hypomania because it can feel like confidence, creativity, productivity, or relief after a low period. This is one reason bipolar disorder can be confused with depression, anxiety, ADHD, substance use, trauma responses, or personality-related concerns.
The goal is not to decide the diagnosis yourself. The goal is to notice patterns clearly enough to describe them to a qualified mental health professional.
Early Signs of Mania and Hypomania
Mania and hypomania can involve elevated, expansive, or irritable mood along with increased energy or activity. Hypomania is usually less severe than mania, but it can still affect judgment, relationships, sleep, and daily functioning.
Signs families may notice
- sleeping much less without seeming tired;
- talking faster or more than usual;
- racing thoughts or jumping between ideas;
- unusual confidence, grand plans, or feeling invincible;
- increased irritability, impatience, or agitation;
- starting many projects at once;
- spending more than usual or making sudden financial decisions;
- riskier driving, sexual behavior, substance use, or travel;
- more conflict, arguments, or sensitivity to limits;
- difficulty slowing down, resting, or accepting concern.
Hypomania can be easy to miss
Hypomania may not look like the stereotype of mania. It may look like high productivity, charm, creativity, confidence, social energy, or intense focus. But if the person is sleeping less, acting out of character, becoming more impulsive, or later crashing into depression, the pattern deserves attention.
If symptoms escalate into unsafe behavior, psychosis, severe agitation, threats, or no sleep for days, use a safety plan. See how to create a bipolar emergency plan.
Early Signs of Bipolar Depression
Bipolar depression can look similar to major depression from the outside. The difference is that it may appear in a larger pattern of mood episodes, including past or future periods of mania or hypomania.
Signs families may notice
- long periods of sadness, emptiness, shame, or hopelessness;
- sleeping too much or struggling with insomnia;
- fatigue, slowed movement, or low motivation;
- loss of interest in people, food, hobbies, sex, or normal routines;
- irritability, anger, or restlessness;
- difficulty concentrating or making decisions;
- missed work, school, parenting tasks, or appointments;
- poor hygiene or not eating normally;
- self-critical language, guilt, or feeling like a burden;
- talk about death, disappearing, or not wanting to exist.
If suicidal thoughts, self-harm language, or immediate danger appears, do not wait for a routine appointment. Seek crisis support. In the United States, call or text 988.
When Highs and Lows Overlap
Sometimes families expect bipolar disorder to look like clear “high” periods and clear “low” periods. In real life, symptoms can feel mixed or confusing. A person may be depressed but also agitated. They may feel hopeless but unable to sleep. They may seem energized but angry, restless, or frightened.
| Possible Mixed Pattern | What It Can Look Like | Why It Matters |
|---|---|---|
| Depression with agitation | Hopelessness, pacing, irritability, insomnia, or intense distress. | This can feel more urgent than quiet sadness and may increase safety concerns. |
| Low mood with impulsivity | Sadness plus spending, substance use, unsafe driving, or sudden decisions. | The family may focus on the behavior and miss the depression underneath. |
| High energy with anger | Less sleep, more activity, conflict, impatience, or verbal aggression. | It may be mistaken for personality or relationship conflict only. |
| Emotional swings with confusion | Rapid shifts, unusual beliefs, paranoia, or disorganized thinking. | Confusion, psychosis, or safety risk needs professional attention quickly. |
What Families Should Track Before an Evaluation
A professional evaluation is easier when the family can describe patterns instead of accusations. Keep notes factual and simple. Avoid writing conclusions like “they are manic” or “they are bipolar.” Instead, write what you saw.
Helpful details to track
- sleep time and wake time;
- days with unusually high or low energy;
- mood changes and how long they last;
- speech changes, racing thoughts, or restlessness;
- spending, driving, substances, sex, conflict, or risky choices;
- missed work, school, parenting, bills, or appointments;
- depressive withdrawal, hopeless words, or self-harm language;
- medication, substances, medical illness, or major stressors if relevant;
- what helped calm the situation;
- what made the situation worse.
If alcohol or drug use may also be part of the picture, read bipolar disorder or drug use: what families can track.
What Else Can Look Like Early Bipolar Disorder?
Many conditions and situations can overlap with bipolar symptoms. This is why families should avoid diagnosing from the outside.
| Could Also Look Like | Why It Can Overlap | What to Do |
|---|---|---|
| Major depression | Low mood, sleep changes, low energy, hopelessness, and withdrawal can overlap. | Track whether there have also been periods of reduced sleep, high energy, or impulsivity. |
| Anxiety | Restlessness, racing thoughts, irritability, insomnia, and panic can look similar. | Ask a clinician to assess the full mood and sleep history. |
| ADHD | Impulsivity, distractibility, restlessness, and emotional intensity can overlap. | Track whether symptoms come in episodes or are more consistent over time. |
| Substance use | Alcohol, stimulants, cannabis, withdrawal, or intoxication can affect sleep, mood, and judgment. | Track substance timing, mood changes, safety risks, and seek qualified support. |
| Trauma or severe stress | Sleep disruption, irritability, emotional reactivity, and avoidance can overlap. | Use trauma-informed, professional support instead of blaming the person. |
| Medical or medication-related causes | Some medical conditions or medications can affect mood, sleep, and energy. | Encourage medical and mental health evaluation, especially if changes are sudden. |
Early Signs in Teens and Young Adults
In teens and young adults, early signs can be hard to separate from normal development, school stress, identity changes, social pressure, or family conflict. The concern grows when changes are intense, repeated, unsafe, or clearly different from the person’s usual pattern.
Families may notice:
- dramatic sleep changes;
- sudden school decline or missed classes;
- intense irritability or conflict;
- bursts of energy followed by crashes;
- risk-taking, unsafe driving, substances, or disappearing;
- long depressive withdrawal;
- talk of death, self-harm, or feeling like a burden.
Diagnosis in children and teens can be complicated because symptoms may overlap with ADHD, depression, anxiety, trauma, autism, substance use, or conduct problems. A careful evaluation by an experienced clinician is important.
If a child or teen is affected by a parent’s symptoms, read supporting children of bipolar parents.
Why Symptoms Can Be Missed in Women and Girls
Bipolar symptoms can be missed in women and girls when the most visible pattern is depression, anxiety, irritability, sleep disruption, emotional sensitivity, or internal restlessness rather than obvious euphoria. Hormonal transitions, pregnancy, postpartum changes, PMDD, perimenopause, trauma, and caregiving stress can also complicate the picture.
This does not mean every mood change is bipolar disorder. It means clinicians need a full history, including sleep, energy, mood episodes, family history, medication reactions, and any past periods of unusual confidence, productivity, impulsivity, or reduced need for sleep.
If your family is worried about hereditary risk, read is bipolar disorder genetic?
When to Seek Professional Help
Consider a professional evaluation when mood, sleep, energy, or behavior changes are repeated, intense, confusing, or affecting daily life. A qualified clinician can assess whether the pattern may involve bipolar disorder, depression, anxiety, ADHD, trauma, substance use, a medical condition, medication effects, or something else.
Seek help sooner if you notice:
- sleeping very little with unusually high energy;
- risky spending, driving, sex, substances, or sudden major decisions;
- depression that lasts, returns, or includes hopelessness;
- psychosis, paranoia, hallucinations, or severe confusion;
- threats, aggression, unsafe behavior, or violence;
- suicidal thoughts, self-harm language, or talk about death;
- symptoms that affect parenting, children, bills, work, school, or safety.
If the person refuses help, read what to do when someone with bipolar refuses help.
How to Talk About What You Are Seeing
Families often want to say, “You are manic” or “You are bipolar.” That usually leads to defensiveness. A safer approach is to describe observations and concern.
| Avoid Saying | Try Saying Instead | Why It Helps |
|---|---|---|
| “You are manic.” | “I noticed you slept two hours for three nights and seem very energized. I am concerned.” | It focuses on observable facts instead of a label. |
| “You are acting crazy.” | “This feels intense, and I want us to slow down and get support.” | It reduces shame and escalation. |
| “You need medication.” | “Would you be open to talking with a qualified clinician about what is happening?” | It avoids giving medical instructions. |
| “Nothing is wrong. You are fine.” | “I may not fully understand it, but I can see this is hard.” | It validates distress without diagnosing. |
| “You are ruining everything.” | “I care about you, and I also need us to protect safety, money, and the kids.” | It separates care from boundaries. |
For more help with wording, read how to communicate with someone who has bipolar disorder and what not to say to someone with bipolar disorder.
What Happens During a Professional Evaluation?
There is no simple home test, blood test, or online quiz that can diagnose bipolar disorder by itself. A professional evaluation may include a detailed conversation about symptoms, sleep, mood history, family history, substance use, medical conditions, medications, trauma, functioning, and safety.
The clinician may ask about:
- episodes of depression;
- periods of unusually high or irritable mood;
- reduced need for sleep;
- impulsivity, risk-taking, spending, or increased activity;
- psychosis or severe confusion;
- family history of mood disorders;
- substance use or medication reactions;
- suicidal thoughts or safety concerns.
If medication is discussed later, read bipolar disorder medication types: what families should know.
Related Guides for Families
- Types of Bipolar Disorder: A Plain-English Guide
- Untreated Bipolar Disorder: Risks and Safe Next Steps
- Bipolar Disorder Medication Types: What Families Should Know
- How to Create a Bipolar Emergency Plan
- Bipolar Disorder or Drug Use? What Families Can Track
- What to Do When Someone With Bipolar Refuses Help
- How to Communicate With Someone Who Has Bipolar Disorder
- Is Bipolar Disorder Genetic?
Trusted Resources
These resources can help families learn more and prepare for professional support. They do not replace individualized medical care.
- National Institute of Mental Health: Bipolar Disorder
- NIMH: Bipolar Disorder in Children and Teens
- Mayo Clinic: Bipolar Disorder Symptoms and Causes
- NAMI: Bipolar Disorder
- SAMHSA: 988 Suicide & Crisis Lifeline
- 988 Suicide & Crisis Lifeline
Frequently Asked Questions About Early Signs of Bipolar Disorder
What are the early signs of bipolar disorder?
Early signs can include sleep changes, unusual energy, racing thoughts, irritability, mood swings, impulsive choices, depression, and periods of high activity followed by crashes. A professional must evaluate the full pattern before diagnosis.
What is usually the first sign of bipolar disorder?
There is no single first sign for everyone. Some people first show depression. Others show reduced need for sleep, unusual energy, irritability, impulsivity, or hypomania that looks like productivity or confidence.
How can families tell the difference between stress and bipolar warning signs?
Stress usually has a clearer trigger and often improves with rest or support. Bipolar warning signs are more concerning when they repeat, intensify, affect sleep and judgment, or cause problems with safety, money, relationships, work, school, or daily life.
Can hypomania look like a good mood?
Yes. Hypomania can look like confidence, energy, creativity, productivity, or social excitement. It becomes more concerning when paired with reduced sleep, impulsivity, irritability, risky choices, or a later crash into depression.
Can bipolar disorder be mistaken for depression?
Yes. Bipolar depression can look like major depression, especially if hypomanic symptoms are subtle or not reported. This is one reason a clinician may ask about past periods of increased energy, reduced sleep, impulsivity, or unusually elevated mood.
Can teens show early signs of bipolar disorder?
Yes, but diagnosis in teens can be complicated because symptoms may overlap with ADHD, anxiety, depression, trauma, substance use, or normal developmental changes. A careful evaluation by an experienced professional is important.
What should families track before an appointment?
Track sleep, mood, energy, speech changes, activity level, spending, risk-taking, substances, depression, missed responsibilities, safety concerns, and how long changes last. Use facts, dates, and examples instead of labels.
When should early signs become urgent?
Seek urgent help if there is suicidal language, self-harm, threats, violence, psychosis, severe confusion, unsafe driving, overdose risk, dangerous substance use, or no sleep for days with escalating behavior.
Should I tell someone they have bipolar disorder?
It is usually better to avoid diagnosing them. Describe what you notice and encourage professional support. For example: “I noticed your sleep, energy, and spending changed a lot this week. I am worried and want us to talk with someone qualified.”
Can early treatment help?
Early professional support can help clarify the diagnosis, reduce risk, build a treatment plan, and support families before symptoms become more disruptive or unsafe.
Final Takeaway
Early signs of bipolar disorder are often easier to see as patterns than as single events. A few nights of poor sleep, one emotional day, or one impulsive decision does not prove bipolar disorder. But repeated changes in sleep, energy, mood, judgment, depression, and safety deserve attention.
Families do not need to diagnose. They can track facts, speak calmly, protect safety, encourage professional care, and get support for themselves too.
The safest next step is simple: write down what you are seeing, watch for risk, and bring the pattern to a qualified professional.